It is important to note that treatment options may vary depending on the type of healthcare system you choose. Not all community hospitals and cancer centers may have the same resources as the academic medical centers commonly found in larger cities.
Wherever you go, your cancer treatment team uses the National Comprehensive Cancer Network (NCCN) cancer treatment guidelines to determine your treatment and care. Your specific treatment options will be based on your cancer’s particular type and stage, location, molecular characteristics, and your overall health. The most common treatments are surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy. Targeted therapy is prescribed for patients with specific types of gene mutations in their tumor. Some patients with specific gene mutations in their tumors may be prescribed targeted therapy drugs.
Surgery
A popular myth about surgery is that the procedure could expose the cancer cells and cause them to spread. This is not true.
Surgery, or having an operation, is the physical removal of the cancer tumor and any nearby lymph nodes that may contain cancerous cells. Ideally, a thoracic surgeon, an expert in lung cancer surgery, should perform this operation. If you need surgery, find a surgical center that performs a lot of lung cancer surgeries. Don’t be afraid to ask whether your recommended surgeon is a thoracic surgeon and how many lung cancer surgeries they have done.
New treatment options are also being tested in clinical trials. If you are interested in learning more about clinical trials, talk with your doctor about the possibility of participating in one. (Click here for more information on clinical trials.)
Questions for my surgeon
- Am I eligible for surgery?
- Can you explain a little about what type of surgery I will have?
- Will my surgery be minimally invasive or open?
- Will lymph nodes be removed?
- How much of my lung will you be taking out?
- How will this affect my breathing?
- Do you anticipate I will need oxygen?
- How long is the procedure?
- How long will I be in the hospital?
- What is the typical recovery time?
- How much pain am I likely to be in afterwards? What can be done to manage it?
- Who should I contact about any side effects I experience? And how soon?
- What are the possible long-term effects of having this surgery?
- Are there treatment options other than surgery for this type of cancer?
- Should I see a medical oncologist or a radiation oncologist?
- Will I need any additional treatment?
Should surgery be part of my treatment plan?
Whether you can be treated with surgery depends on:
- the type and stage of your cancer. If your cancer has spread to other organs, such as the case in stage 4, surgery is generally not recommended.
- the location and size of your tumor. If the surgeon cannot safely remove your tumor, the disease is called inoperable, or unresectable, and surgery may not be an option (stage 3B, stage 4 and some stage 3A NSCLC).
- if you are otherwise healthy enough to have surgery. If you have heart or lung disease in addition to lung cancer, you may not be able to withstand surgery.
Recovery times are different for everyone
Just as many factors influence whether you have surgery, there are factors that will influence how long it takes for recovery. Recovery time will vary depending on your particular surgery, your general health, and how well you heal.
Open surgery: If you have lung cancer surgery through the traditional, opened-chest approach, full recovery usually takes 6 to 8 weeks.
Less invasive surgical approaches: Depending on the size and location of your tumor, you may be able to have lung surgery by a minimally invasive approach, either video-assisted thoracic surgery (VATS) or robotic-assisted thoracic surgery (RATS). This type of surgery is less invasive because it uses smaller openings and a video camera to guide the surgeon. This procedure results in less injury to your bones and muscles, and possibly a shorter recovery time.
Types of surgery
(May be done openly or, in some cases, by minimally invasive surgery)
Lobectomy
The entire lobe (portion) of the lung affected by lung cancer is removed. The right lung has three lobes, and the left lung has two, so having a lobectomy allows you to maintain most of your lung function. This is generally the preferred procedure, although it depends on your unique situation.
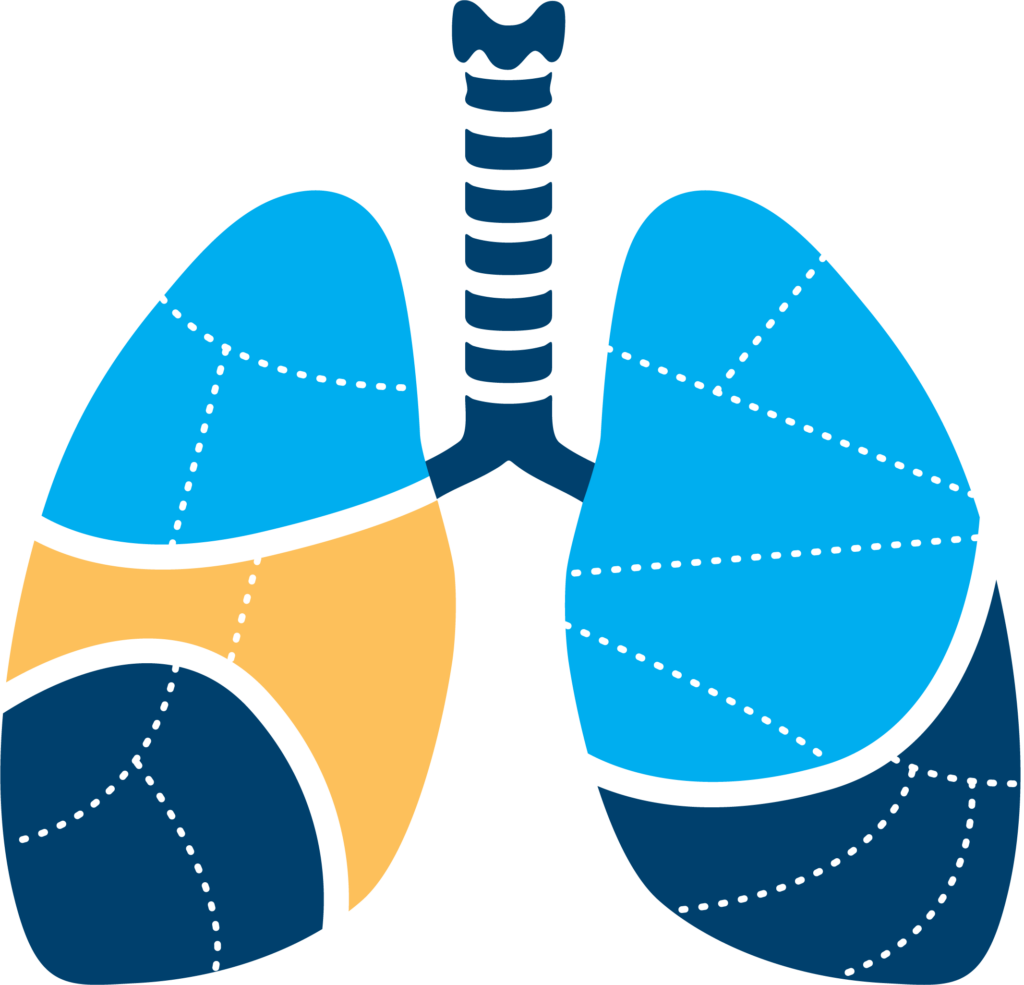
Segmentectomy
One or more segments (regions supplied by distinct blood and air supply) of the lung that is affected by the lung cancer are removed. Typically, the amount of lung tissue and lymph nodes removed in a segmentectomy is more than in a wedge resection, but less than in a lobectomy.
Wedge resection
The surgeon removes a small wedge-shaped section of the lung containing the tumor and a small amount of healthy tissue around the cancer. This procedure allows you to maintain a majority of your lung function.
Pneumonectomy
The surgeon completely removes the lung with cancer. This must be done when the tumor is located in the lung’s largest airway or very near the trachea (windpipe), or when the cancer affects more than one lobe of the lung. This procedure can significantly reduce lung function, but most people find they can get back to nearly normal activities with the help of physical and respiratory therapy.
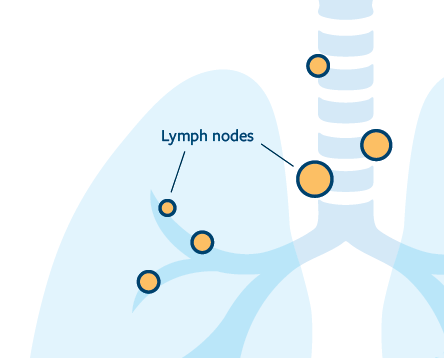
Removal of lymph nodes
If you have surgery, your surgeon will likely also remove some lymph nodes from the lung and the center of the chest (your mediastinum) to check them for cancer cells. This can be done as a separate procedure prior to your operation, or during the operation itself. This will help your doctors determine if your cancer has spread elsewhere in your body and may change your staging and treatment plan. You may be a candidate for chemotherapy, immunotherapy, and/or targeted therapy before (neoadjuvant) or after (adjuvant) surgery. This is dependent on the stage of your cancer and the presence of molecular markers.
Radiation therapy
Radiation therapy (also referred to as radiotherapy, x-ray therapy, or irradiation) is the use of x-rays or other high-energy beams (such as protons) to target cancer cells and stop them from growing or multiplying so that they eventually die. Radiation treatment machines are directed to the tumor and the surrounding area and are “on” for a few minutes, delivering radiation that can kill tumor (as well as normal) cells. Sophisticated radiation planning can help to spare the normal tissues from exposure to radiation to selectively kill cancer cells. Like surgery, radiation is a local form of therapy and not a systemic (whole-body) treatment like chemotherapy or targeted therapy. High doses (amounts) of radiation are given when the tumor is confined to one area of the body, with the hope that the radiation will kill all of the tumor cells in that area. This treatment might involve daily doses of radiation for as little as one day or as much as six weeks or longer. Your physician will determine the best course of action for your tumor.
If the cancer has spread from the lungs to other parts of the body, radiation may be given in an abbreviated course to relieve symptoms in affected areas, such as the brain, lungs or bones. Radiation given for periods ranging from one day to four weeks can kill enough cancer cells to bring relief from symptoms such as pain, breathing difficulties, and headaches.
Specialized radiation therapy
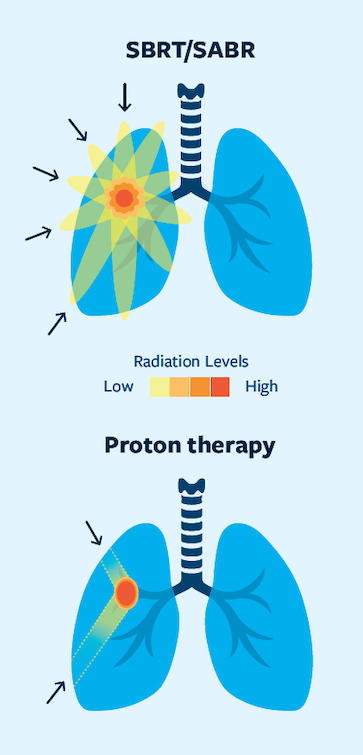
Your radiation oncologist may recommend a special type of treatment called Stereotactic Body Radiation Therapy (SBRT) or Stereotactic Ablative Radiotherapy (SABR); these terms mean the same thing. SBRT/SABR uses radiation from multiple angles, which allows higher doses of radiation to be precisely focused on the tumor, avoiding as much healthy tissue as possible. SBRT/SABR can be used to treat some localized tumors in people who cannot have surgery due to other health conditions or to treat some tumors that cannot be surgically removed because they are in a difficult location. SBRT/SABR can be performed with many different types of machines, and different options may be presented to you depending on the machines available at a given treatment location. Cyberknife® is the brand name for a system that uses high-precision radio surgical and SBRT procedures.
A very focused form of radiation therapy, called stereotactic radiosurgery, or SRS is sometimes offered if the cancer has spread to the brain or bones. This type of radiation therapy might be given in only one session. It can be used instead of or along with surgery for single tumors that have spread to the brain. Gamma Knife® is one example of a machine that focuses radiation on the tumor from different angles.
Proton therapy
A specialized form of radiation therapy uses protons to deliver the radiation to the patient. Unlike traditional radiation (known as photons or x-rays), protons do not give radiation to tissue beyond the target area. Consequently, they have the potential to uniquely spare your healthy tissues. The use of proton-based radiation is being actively explored in lung cancer but is not currently a standard approved therapy.
Chemotherapy
Chemotherapy drugs are medications that travel through the bloodstream to kill cancer cells throughout the body. These drugs are administered through the veins via an IV or through a mediport, or rarely, taken orally as pills. Unlike surgery and radiation, which are used to treat disease locally, chemotherapy is systemic; it can affect cancer cells throughout the body.
Keep in mind that chemotherapy is not always used with every patient – chemotherapy is a medication that some people receive as first or second line therapy in their treatment journey for lung cancer. It may differ for you or your loved one.
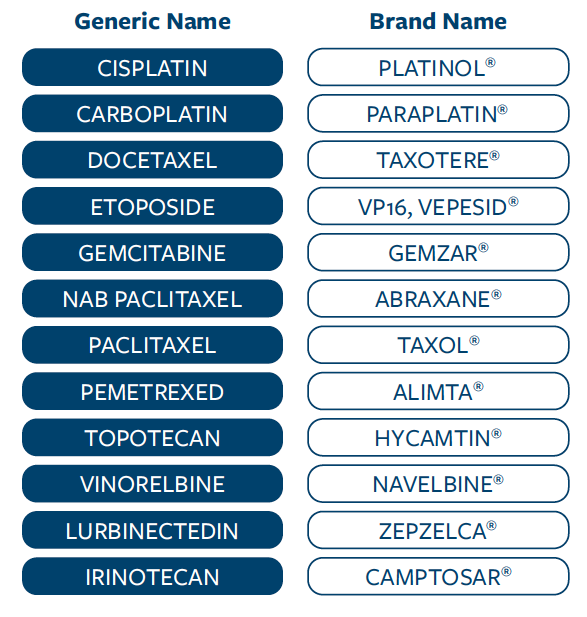
A number of different chemotherapy drugs are used for lung cancer, including the following. (Updated March 2026)
Generally, one platinum-containing agent (cisplatin or carboplatin) is combined with a non-platinum drug. Additional or different combinations of therapies may be prescribed by your doctor depending on their expert opinion on what is likely to work best for you. Still more drugs are in development, and these may be available after the printing of this booklet.
It is important to know that different types of cancers are treated with different types of chemotherapy, and that chemotherapy has changed a lot over the years. If someone tells you what they or a friend went through, remember that your cancer and your treatment — and therefore your experience — may be very different. See this link for some possible side effects of chemotherapy and other treatments, and ways to manage these symptoms.
Targeted therapy
One way in which cancer cells differ from normal cells is that they often have abnormalities (such as mutations and fusion proteins) in their DNA. To help fight cancer, scientists have developed drugs that specifically target cancer cells that have these mutations. By targeting mutations of cancer cells, these drugs can stop or limit the growth and spread of cancer. These drugs are also called “molecular targeted therapies/drugs” or “precision medicines” because they precisely target the mutation that is causing the cancer. Targeted therapies usually come in the form of pills but may also be other types of IV or subcutaneous (under the skin) preparations too.
As of June 2026, the targeted therapies approved to treat NSCLC are:
| Gene | FDA-Approved Drugs* |
|---|---|
| ALK | Alectinib (ALECENSA®) Brigatinib (ALUNBRIG®) Ceritinib (ZYKADIA®) Crizotinib (XALKORI®) Ensartinib (ENSACOVE™) Lorlatinib (LORBRENA®) |
| BRAF | Dabrafenib (TAFINLAR®) + trametinib (MEKINIST®) Encorafenib (BRAFTOVI®) + binimetinib (MEKTOVI®) |
| EGFR | Afatinib (GILOTRIF®) Amivantamab-vmjw (RYBREVANT®) + lazertinib (LAZCLUZE™) Dacomitinib (VIZIMPRO®) Datopotamab deruxtecan-dlnk (DATROWAY®) Erlotinib (TARCEVA®) Gefitinib (IRESSA®) Osimertinib (TAGRISSO®) |
| EGFR Exon 20 | Amivantamab-vmjw (RYBREVANT®) + chemotherapy Sunvozertinib (ZEGFROVY®) |
| HER2/ERBB2 | Sevabertinib (HYRNUO®) Trastuzumab deruxtecan (ENHERTU®) Zongertinib (HERNEXEOS®) |
| KRAS G12C | Adagrasib (KRAZATI®) Sotorasib (LUMAKRAS®) |
| MET | Capmatinib (TABRECTA®) Telisotuzumab vedotin (EMRELIS™) Tepotinib (TEPMETKO®) |
| NRG1 | Zenocutuzumab (BIZENGRI®) |
| NTRK | Entrectinib (ROZLYTREK®) Larotrectinib (VITRAKVI®) Repotrectinib (AUGTRYO™) |
| RET | Pralsetinib (GAVRETO®) Selpercatinib (RETEVMO®) |
| ROS1 | Crizotinib (XALKORI®) Entrectinib (ROZLYTREK®) Lorlatinib (LORBRENA®)† Repotrectinib (AUGTYRO™) Taletrectinib (IBTROZI™) |
Because targeted therapies work best for people whose tumors have a specific gene mutation or changes, testing your tumor is very important. These tests can be called molecular, biomarker, genetic or mutation testing. Testing for a protein called PD-L1 may be helpful in deciding about immunotherapy treatment.
Some doctors recommend another biopsy or a blood test (liquid biopsy) to see if your tumor has shown other causes of resistance. Many drugs are being developed specifically for patients whose tumors have developed resistance. Biomarker testing is often needed to see if you are eligible for clinical trials of targeted therapies that address resistance issues.
Drugs are getting approved very rapidly, and the list will be changing. If there’s a drug that isn’t on this list, please ask your doctor about it. A lot of drugs still under development may be approved soon. Some may even be used in combination with other treatments (such as osimertinib plus chemotherapy, or amivantamab plus chemotherapy).
Monoclonal antibodies
Antibodies are important parts of our immune system. As proteins, they can bind to and help fight off viruses and cancer cells. Each monoclonal antibody binds to only one antigen (foreign substance).
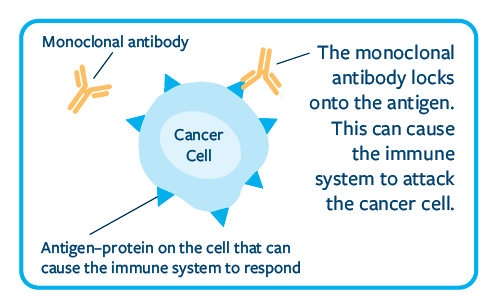
Important research has helped with discoveries in this area. Scientists can now make a type of monoclonal antibody that can bind to the abnormal proteins made by cancer cells.
Antibodies can bind to these abnormal proteins and stop them from becoming activated.
The abnormal proteins that cancer cells can make are:
- PDL and PD-L1 (see Immunotherapy section)
- EGFR (see Biomarker Testing section)
- VEGF (Vascular Endothelial Growth Factor)
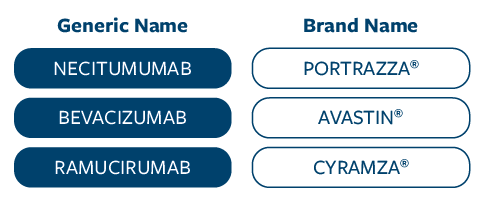
As of March2026, the monoclonal antibodies approved to treat NSCLC (other than those listed under immunotherapies in the next section) are:
Immunotherapy
Immunotherapy is one of the most exciting new approaches for treating lung cancer.
Immunotherapies work by boosting your body’s own natural defenses to fight cancer.
The immune system is the body’s defense against disease. It has the ability to recognize and destroy not only infections like bacteria and viruses, but also abnormal cells like cancer cells. But cancer cells are sometimes able to hide from or weaken the immune system, so they are not recognized and not destroyed. If cancer cells escape the immune system, they can continue to grow and spread. Scientists have been making breakthrough discoveries about how cancer cells evade the immune system. These discoveries have led to new therapies that may stimulate the immune system to attack cancer or counteract the ways cancer cells hide from or suppress the immune system.
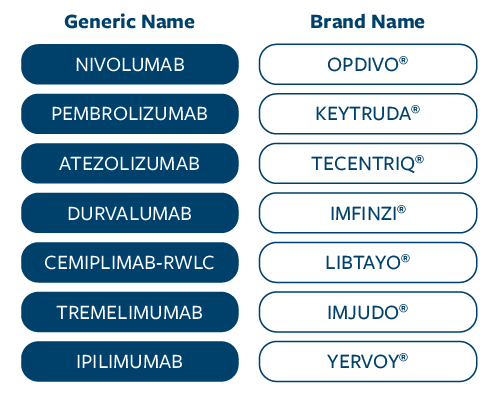
As of March 2026, the immunotherapies approved to treat NSCLC are:
These immunotherapies are given into the vein (intravenously or IV) and some can also be given under the skin (subcutaneously or SQ). They differ in how often they are given.
Because immunotherapy drugs work on the immune system, they work differently from chemotherapy. The side effects of immunotherapy drugs are also different from those of chemotherapy. The most common side effects patients experience with immunotherapies can include diarrhea, fatigue, itching, skin rashes, muscle, joint, or bone pain, nausea, shortness of breath, and pneumonitis. Rarely, these drugs can cause the immune system to become too active. This may cause the body to react against normal tissues, such as your lungs, liver, colon, or thyroid.
More immunotherapies are being developed and tested in clinical trials for a variety of lung cancer
types and stages. For SCLC, the T cell engager tarlatamab is a BiTE (bispecific T cell engager) that is approved for second-line treatment.
Keep in mind that immunotherapy for lung cancer is still new and research to figure out how best to use them – and which people are most likely to benefit – is ongoing. Ask your doctor if immunotherapy treatments or clinical trials might be options for you.
Antibody Drug Conjugates (ADCs)
ADCs are agents that target a protein (antigen) on the cancer cell and directly deliver the chemotherapy or payload.
Three ADCs are currently approved: trastuzumab deruxtecan for HER2 altered NSCLC, telisotuzumab for NSCLC with high c-MET expression, and datopotamab deruxtecan for EGFR mutated NSCLC after prior therapy.
Tumor Treating Fields (TTFs)
Tumor Treating Fields are delivered through a wearable device that alternates electrical currents to disrupt cancer cells. Optune Lua® is the brand name for the TTF device that is FDA approved as second-line treatment, usually in combination with immunotherapy or chemotherapy.
Talk with your doctor about whether you may be a candidate for this treatment, and discuss the potential side effects and benefits associated with its use.
Small cell lung cancer (SCLC) treatments by stage
Limited stage
Limited-stage SCLC is typically treated with radiation to the chest, chemotherapy, immunotherapy, or PCI*.
Extensive-stage
Individuals with extensive‑stage SCLC are treated with chemotherapy, immunotherapy, or PCI*.
* Prophylactic cranial irradiation (PCI), radiation to the whole brain used to prevent brain metastases, may also be discussed at either of these stages
Non-small cell lung cancer (NSCLC) treatments by stage
Because new treatments are rapidly becoming available, we’ll do our best to keep this list up-to-date. However, please speak with your doctor if you have any questions on available treatment options.
Preferably, treatment decisions will be guided by a multidisciplinary team. Your input as the patient is essential. These conversations are part of the shared decision-making process between you and your team.
Stage 1
The ideal treatment for stage 1 NSCLC is surgery to remove the tumor. New research is helping doctors predict which patients with stage 1 NSCLC will need chemotherapy, immunotherapy, or targeted therapy before or after their surgery and which will not. High-dose radiation therapy may also be used if you or your doctors feel that you would not tolerate surgery (see page 14 for more information). Osimertinib is approved as adjuvant (see glossary) therapy in stage 1B-3A EGFR mutated lung cancer and alectinib is approved for ALK positive lung cancer. Research is ongoing to determine if other targeted therapies should be given as well.
Stage 2
Optimal treatments for stage 2 NSCLC are chemotherapy and immunotherapy followed by surgery, surgery followed by chemotherapy and immunotherapy, or targeted therapy. Osimertinib is approved as adjuvant therapy for EGFR mutated lung cancer stage 1B-3A, and alectinib is approved for ALK positive cancer. Research is ongoing to determine if other targeted therapies should be given as well.
Stage 3
Treatment options may differ depending on the extent of the disease. Although surgery is generally not recommended for stage 3 lung cancer, it may be considered in specific cases for patients with stage 3A disease. In these cases, chemotherapy and immunotherapy may be used prior to surgery. Treatment for most patients with stage 3 NSCLC who do not receive surgery usually includes chemotherapy, radiation therapy, and immunotherapy. Chemotherapy and radiation therapy may be given at the same time or one after the other. Immunotherapy is typically given after a combination of chemotherapy and radiation therapy. Osimertinib is approved as adjuvant therapy for EGFR mutation positive lung cancer after completion of chemotherapy and radiation. Research is ongoing to determine if other targeted therapies should be given as well.
Stage 4
Chemotherapy is often used because it fights the cancer throughout the body. Sometimes immunotherapy is given with it, or depending on one’s PD-L1 status, immunotherapy may be given alone. Targeted therapy may be used alone if one’s tumor has a positive biomarker. Radiation may be used to shrink tumors that are causing symptoms. Because stage 4 cancer has spread to other parts of the body, surgery is only recommended in very select cases. Other treatment options may be available, and these should be discussed with your oncologist.