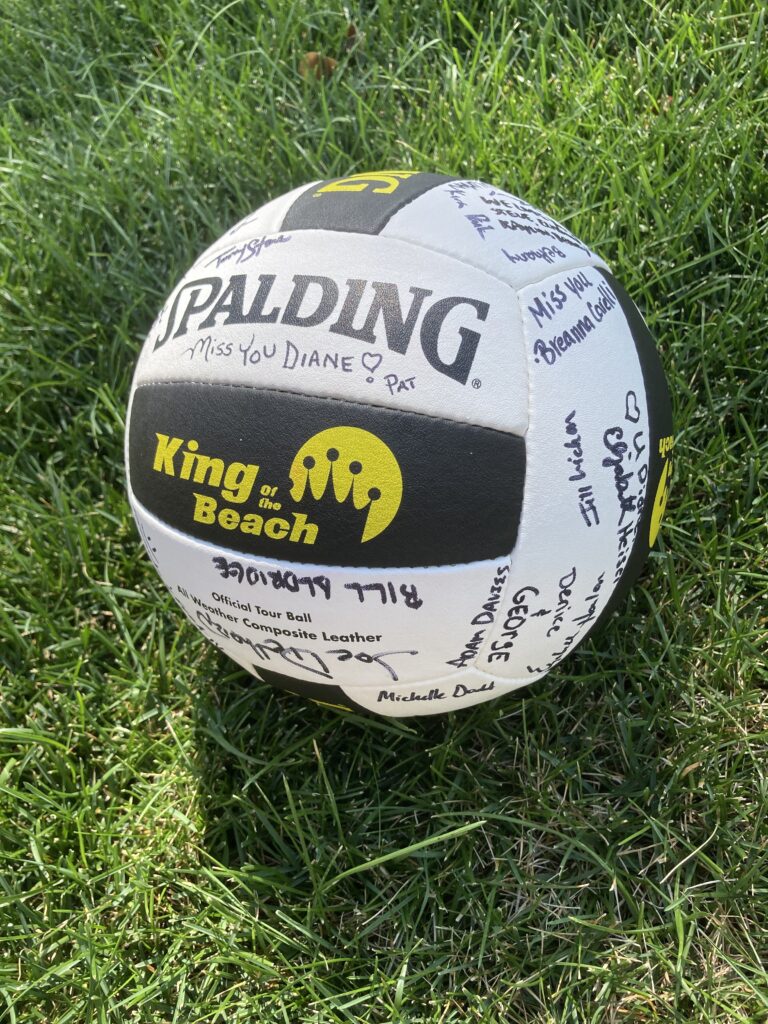
When Janae Bowie decided she wanted to hold a fundraiser in memory of her mother, Diane Minnick, volleyball rose to the top of the list.
Diane was diagnosed with non-small cell lung cancer in March 2020 at 61 years of age and passed away in December. Janae describes her as “a very caring, loving and selfless woman who always put others before herself. She touched many hearts in her community.” She also loved sports, including biking, playing pickle ball, and especially volleyball.
Diane’s cancer had the EGFR mutation, and Janae’s fundraiser went towards the EGFR Resisters/LCRF partnership to raise funds for new EGFR-positive lung cancer research projects. The memorial volleyball tournament took place Aug. 22 in Westminster, CO, and so far, has raised over $7,700.
Thank you to Janae, her family and friends for all their hard work and efforts into making this fundraiser a success!
LCRF board member Colleen Conner Ziegler was quoted in an article about lung cancer screening on BlackDoctor.org. She talked about her own experience of when she received a diagnosis of advanced lung cancer at age 58.
“It took a visit to the hospital after coughing up blood to receive an accurate diagnosis after a chest X-ray and CT scan revealed a mass in my lungs,” she said. “That is why as a cancer community we need to educate on risks and symptoms of the disease, especially in underserved populations, because lives truly depend on it.”
As fall 2021 approaches, we’ve seen a number of interesting developments in lung cancer research in the year so far.
Several new findings were introduced at the American Association for Cancer Research (AACR) and American Society for Clinical Oncology (ASCO) annual meetings. Another major conference, the International Association for the Study of Lung Cancer (IASLC) World Conference on Lung Cancer, will take place Sept. 8-14.
To read the more comprehensive version of this update, click here.
Targeted therapies
Targeted therapies continue to be an area of potential new development.
Dr. Eugene Manley, Jr.
“Roughly, about 9-10 key driver mutations for lung cancer – specifically non-small cell lung cancer – are likely to indicate disease progression. A lot of the work presented at these national summits talked about some of the key developments in targeting these mutations,” said Eugene Manley, Jr., PhD, LCRF’s Director of Scientific Programs.
“We’ve learned about tumor biology and keep learning more,” he added. “Many tumors are what we call heterogeneous, which means they don’t all have the same types of cells.” This results in cells with different protein expression, gene expression, and even different transcription factors that affect how the cells grow, how they respond to therapies, and whether they might be sensitive to or resist therapies.
LCRF played a role in making molecular profiling standard of care during the 2nd iteration of the Lung Cancer Mutation Consortium. The 4th iteration, the LCRF LEADER trial, will soon be underway and will look at treatment in a neoadjuvant setting.
Dr. Kathryn Gold, UCLA
Kathryn Gold, MD, LCRF’s guest for July’s #TogetherSeparately Lung Cancer Mid-Year Update webinar, provided context on new drugs and targeted therapies, as well as disparities, drug resistance and the impact on patients. (Click here to view the webinar recording.)
“Because research has moved fast, we have a lot of approved therapies right now that have never been directly compared to each other, and that can make it kind of difficult to figure out what the best is for any one person,” Dr. Gold stated. As an example, she noted that five FDA approved drugs are available for patients with ALK-positive lung cancer: crizotinib, ceritinib, alectinib, brigatinib, and lorlatinib. While clinical trials have shown that the four newer drugs are likely more effective than crizotinib, “they’ve never been compared head-to-head versus each other,” she said. “So when I am seeing that brand-new diagnosis of ALK-positive lung cancer in a patient in my clinic, I have five options, which is great, but I don’t have anything to tell me which one is best.”
However, Dr. Gold noted that too many options is better than not having enough. “It’s a good problem to have,” she said.
The J-ALEX study compared alectinib and crizotinib in patients with the ALK mutation. “Earlier time points showed that alectinib treatment let to increased overall survival and progression-free survival, but the five-year data only showed better progression-free survival, not an increase in overall survival,” Dr. Manley said. “You get more time without the tumor returning, but in essence survival rates aren’t different after five years.” Having multiple drugs to target a mutation opens the possibility of using each drug successively. The CROWN study showed that in advanced ALK+ NSCLC, lorlatinib was much better than crizotinib for increasing progression-free survival rates and decreasing brain metastases.
EGFR is one of the most common mutations in non-small cell lung cancer. Osimertinib (Tagrisso) was granted FDA approval in December 2020 for EGFR-mutant NSCLC based on the ADAURA trial. In this trial, patients whose tumors tested positive for the EGFR mutation received either osimertinib or the previously standard care of regular CT scans with monitoring. While osimertinib reduced the risk of the tumor returning, it’s unclear whether the drug will help people live longer.
As Dr. Manley noted, “The results are significant because they made osimertinib the first personalized therapy in the adjuvant setting, and it can be used for early-stage patients with EGFR-positive lung cancer.”
Patients eventually develop resistance to osimertinib, and several trials had encouraging results targeting osimertinib-resistant NSCLC. In the CHRYSALIS trial, amivantamab combined with orally delivered lazertinib was shown to subsequently impede tumor growth. Another trial points to patritumab deruxtecan (HER3-DxD), an antibody drug conjugate (ADC), as a potential option. In an ADC, the antibody is used to home in on the tumor while attached to a chemotherapy drug. This approach is thought to more specifically target the tumor while minimizing systemic exposure or toxicity.
Patients with EGFR Exon 20 insertion mutations whose cancer had advanced on chemotherapy now have their first targeted therapy option. In May, the FDA approved amivantamab (Rybrevant), a monoclonal antibody delivered intravenously, to treat this rare mutation. This antibody had an unprecedented 40% response rate, increased survival rates, and was well tolerated.
The FDA granted the oral medication poziotinib Fast Track designation in March for use in patients with EGFR and HER2 Exon 20 mutations. While response rates are high for this drug, toxicity is a concern.
While KRAS is the most frequent mutation, found in 20-40% of NSCLC patients, the specific KRAS G12 mutation was thought to be undruggable until the FDA’s recent approval of sotorasib (Lumakras®). Sotorasib was found to be safe while shrinking tumors and improving survival for patients with this mutation who had previous systemic. A chemically similar therapy, adagrasib (MRTX849), was given FDA Breakthrough designation in June.
Other findings:
The combination of pertuzumab, trastuzumab, and docetaxel reduced tumor growth in patients with metastatic NSCLC with HER2 Exon 20 mutation.
After a COVID screening led to a patient’s NSCLC diagnosis, liquid biopsy was used to identify their cancer as RET-fusion positive. Treatment with selpercatinib (Retemvo) reduced the patient’s tumor mass.
The ARROW study showed that orally delivered pralsetinib (Gavreto) had strong antitumor activity in patients with advanced solid tumors harboring RET fusions, including NSCLC.
The GEOMETRY mono-1 trial showed that capmatinib is effective for MET Exon 14 (METex14) skipping NSCLC patients as a first-line therapy.
The VISION trial used tepotinib as treatment for patients with MET Exon 14 mutations detected with a Guardant360™ liquid biopsy. Tepotinib had some efficacy in patients with MET amplified NSCLC, which was a continuation of their results from an earlier study.
While more and more breakthroughs are happening around targeted therapies, not every patient’s cancer is being tested for multiple biomarkers.
The MYLUNG Consortium showed that in community-based settings, many in the southeastern US, 90% of tumors are tested for at least one of the most common biomarkers – ALK, BRAF, EGFR, ROS1, and PD-L1. But only 46% were tested for all five biomarkers prior to therapy, which means patients may not be receiving appropriate clinical trials or therapies.
“We’ve made it a lot of advances in the past 15 years, and I don’t think any of those would be possible without profiling of tumors,” said Dr. Gold. “Every single person with adenocarcinoma of the lung should get mutational profiling. And I think they should get a pretty broad panel, not only for EGFR, KRAS, ALK, but for all those less common ones, as well.”
Disparities in health care access continue to be an issue. The FLATIRON health database retrospective study showed that while there was no difference between white and Black patients in gene alterations, Black patients were 10% less likely to receive biomarker testing in general and 7% less likely to receive it before targeted therapy. Some of the barriers to testing include tissue limitations, provider education, and patient access. These differences also manifested in access to and enrollment in clinical trials, where white patients were twice as likely to be enrolled than Black patients.
“The biggest problem with that is if you don’t know what driver mutation they have before you start therapy, you may make it much worse,” Dr. Manley explained. “You could give them a drug they’re resistant to because of a mutation that you didn’t test.”
LCRF and the AME Church Health Commission announced a partnership this spring to increase lung cancer awareness, education, and screening in Black Americans to reduce mortality rates.
Immunotherapy
“Some really interesting data with immunotherapy and early-stage lung cancer was presented at ASCO,” Dr. Gold noted. Immunotherapy uses drugs “that try to persuade your body’s immune system to attack the cancer,” she explained. “It’s very commonly used in Stage IV lung cancer, and also in Stage III lung cancer after radiation, but had not yet been used in early stage lung cancer.”
The IMpower 10 trial studied a PD-L1 inhibitor, atezolizumab, in people who had lung cancers that were resected surgically and then treated with chemotherapy. The patients were randomized to either immunotherapy or standard of care, which was observation.
“Like the ADAURA trial showed, what we saw in this trial was that it did seem to reduce the risk of the tumor coming back,” Dr. Gold explained.
Watch Dr. Gold’s #TogetherSeparately mid-year update
Several other studies looked at combining chemotherapy and immunotherapy.
The Checkmate 816 trial compared nivolumab and platinum-doublet chemotherapy with chemo alone in patients with resectable NSCLC. Results showed that after four years, the combination was more effective at improving survival than chemotherapy alone in the neoadjuvant setting.
The two-year update for the Checkmate 9LA trial showed improved survival for patients with advanced NSCLC treated with a combination of nivolumab, ipilimumab and two cycles of chemotherapy, compared with treated four cycles of chemotherapy alone. This suggests that the combination therapy is effective as a first-line treatment option.
The Checkmate 227 trial presented four-year follow-up data of patients with advanced NSCLC with expression of PDL1 ≥ 1% or < 1% treated with nivolumab, ipilimumab, or the two drugs together. The combination was more effective in patients with both PD-L1 ranges compared to the solo therapies.
The FDA analyzed clinical trial data of approved therapies for advanced NSCLC patients with PD-L1 (1-49%) treated with immunotherapy alone or the combination of chemotherapy and immunotherapy. The combination led to better survival rates than immunotherapy alone as a first line treatment, but since these trials included a disproportionately low number (2%) of Black patients, we can’t conclude whether treatment will be effective in that population.
The PACIFIC trial presented a five-year update on patients with unresectable stage III NSCLC that had progressed following chemotherapy. The combination of durvalumab (Imfinzi) and chemoradiation increased overall survival and disease-free survival compared to the placebo.
NSCLC patients with high Tumor Mutational Burden (TMB) have a higher overall response rate and greater overall survival with immune checkpoint inhibitors when compared to those with intermediate or low TMB.
The use of antibiotics before or at the start of immune checkpoint inhibitors is associated with worse overall survival, which does not occur with chemotherapy.
Small Cell Lung Cancer
“With small cell lung cancer, it is still not the standard for patients to get profiling,” said Dr. Gold. “That’s unfortunately because most of the mutations that we find in small cell are not things that we know how to target with the medications that we have available to us right now.”
Recent work has showed that SCLC is not one distinct tumor but has several subtypes of cells that can be categorized into five groups: SCLC-A, SCLC-N, SCLC-P, and SCLC-I. SLCL-I is inflamed, which may predict sensitivity to immunotherapies. Other subtypes are linked with drug resistance.
Another group characterized these subtypes as SCLC-A, SCLC-N, SCLY-Y, SCLC-P, and SCLC-Mixed; and a third group identified three subtypes and found a marker, PLCG2, that may be associated with more metastatic tumors and worse outcomes.
Dr. Gold thinks that the future will bring more questions. For example, “drugs like sotorasib seem to work pretty well as a single agent. Can we make it better by combining it with immunotherapy? By combining it with chemotherapy? Maybe even moving it to the frontline setting? Those are the things that we’ll be talking about in a year. We have little teases of that data right now, but a year from now, I think we’ll have a lot more kinds of concrete data.”
Dr. David P. Carbone was our guest Aug. 18 for a #TogetherSeparately live talk on Why Biomarker and Genomic Testing Matters.
During the livestream, Dr. Carbone talked about the promise and successes of targeted therapies and immunotherapy, answered questions about oncogene mutations and available treatments, and outlined current studies that could be game-changers for lung cancer patients. Watch the video below.
LCRF Scientific Advisory Board member Dr. John Minna co-led a study that could potentially shape the fight against cancer drug resistance.
The study at UT Southwestern explored using lentiviruses to purposely mutate genes that produce cancer-driving proteins. This process could help scientists understand the resistance that inevitably develops to targeted therapies.
Dr. Carbone tells USA TODAY: nonsmokers can get lung cancer
USA TODAY reached out to Dr. David Carbone, director of the James Thoracic Oncology Center at Ohio State University, for an expert opinion on lung cancer risk. He pointed out that people who do not smoke tobacco products can still be at risk of developing lung cancer.
Dr. David Carbone
“Among lung cancer circles, what we say is if you have lungs, you can get lung cancer,” he said.
Dr. Carbone is a member of LCRF’s Scientific Advisory Board and the featured guest for August’s #TogetherSeparately Lung Cancer Community Talk on the topic, “Why Biomarker and Genomic Testing Matters.”
LCRF Board Chair co-authors commentary on adjuvant trials for resected NSCLC
Posted July 15, 2021
Dr. Brendon Stiles
LCRF Board Chair Dr. Brendon Stiles co-authored a commentary published recently in The Journal of Thoracic and Cardiovascular Surgery on adjuvant trials for patients with resected non-small cell lung cancer (NSCLC). They noted that surgeons lead the care of early stage NSCLC patients and concluded that they need to know the trial data and insist on comprehensive biomarker testing.
Source: Chudgar NP, Stiles BM, Commentary: Adjuvant Therapy in Resected T1-2N0 NSCLC: Surgeons Should Lead, The Journal of Thoracic and Cardiovascular Surgery (2021), doi: https://doi.org/10.1016/j.jtcvs.2021.07.006.
SAB member talks about adjuvant therapy’s potential for treating early stage NSCLC
Posted June 23, 2021
CancerNetwork® interviewed LCRF Scientific Advisory Board member Suresh S. Ramalingam, MD at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting on a trial involving atezolizumab (Tecentriq) in early-stage non–small cell lung cancer (NSCLC). He talked about the potential this and other trials involving adjuvant therapy have for early disease.
Panelist speaks on overcoming drug resistance in SCLC
Posted May 21, 2021
Dr. Kwok-Kin Wong
LCRF grantee Dr. Kwok-Kin Wong was part of a panel on combination approaches to overcome drug resistance during the American Association for Cancer Research (AACR) Annual Meeting this week.
Dr. Wong described the development of the next generation CDK7 inhibitor YKL-5-124 and its application to small-cell lung cancer (SCLC) as a single agent and in combination with chemotherapy and immune checkpoint inhibitors.
Immune-boosting drug could help before lung cancer surgery
Posted April 20, 2021
Doctors have reported that a drug that helps the immune system fight cancer gave dramatic results when used with chemotherapy before lung tumor surgery. Nivolumab (Opdivo®) is a checkpoint inhibitor which helps the immune system find some types of cancer cells that are hidden. Checkpoint inhibitors are often used after cancer surgery, and are being tested before surgery as well.
Dr. Roy Herbst, lung specialist at the Yale Cancer Center and a member of LCRF’s Scientific Advisory Board, commented on the reports: “They open the person up and the tumor’s just melted away. It’s incredible.”
A new publication surveyed pathologists around the world on their methods of detecting the PD-L1 biomarker in non-small cell lung cancer patients.
PD-L1 is a protein that, in some cancers, is produced in abnormally large amounts. This prevents the immune system from detecting the cancer cells, allowing them to survive.
Since PD-L1 is a predictive biomarker, patients who have tumors with high PD-L1 staining can be treated with pemblolizumab (Keytruda®). The survey showed variability in PD-L1 antibodies, testing procedures, tissue processing, analysis time, and quality control. This suggests that there is a need for standardization to ensure patients’ benefit. However, the costs associated with antibodies, instrumentation, and specific training may be barriers.
Phase II trial shows improved outcomes for elderly EGFR+ NSCLC patients
Posted April 1, 2021
A recent small Phase II trial out of Japan showed that elderly patients with EGFR mutation-positive non-small cell lung cancer treated with the EGFR inhibitor, Afatanib (Gilotrif®), as a first-line therapy had significantly improved outcomes and survival rates. Some patients still needed to have the dose lowered, but this is a positive observation.
New guidelines make more people eligible for yearly lung cancer screening
Posted March 9, 2021
New guidelines by the U.S. Preventive Services Task Force will nearly double the number of people in the United States who are advised to have yearly CT scans to screen for lung cancer.
The new recommendations include people ages 50 to 80 who have smoked at least a pack a day for 20 years or more, and who still smoke or have quit within the past 15 years. This lowers the age when screening should start from 55 to 50, and reduces the smoking history from 30 years to 20. The change means many more African-Americans and women will be eligible for screening than in the past.
Disparities in lung cancer screening may persist despite revisions to USPSTF guideline
Posted March 3, 2021
The U.S. Preventive Services Task Force changed their guidelines for lung cancer screening to allow those who are younger and smoke less to be eligible. While their goal was to help reduce the lung cancer screening disparity we see in women, specifically Black and Hispanic women, researchers are critical of how much it will help. Raising or lowering the criteria based on age and smoking history are unlikely to have a meaningful effect on reducing inequities. Lung cancer screening criteria are likely to remain biased unless they are adjusted for different racial/ethnic groups.
The KEYNOTE-010 study evaluated the use of either pembrolizumab or docetaxel in patients with previously treated, PD-L1–positive advanced non–small cell lung cancer. LCRF Scientific Advisory Board member Dr. Roy S. Herbst talked about what multidisciplinary care teams can take away from this research.
Targeted treatment shows promise for brain metastases in EGFR+ NSCLC
Posted February 11, 2021
Early stages of a clinical trial studying the targeted treatment osimertinib is showing promise for patients with brain metastases with EGFR+ non-small cell lung cancer (NSCLC). Patients in the study showed a reduction in brain metastases volume after the treatment was completed. Osimertinib is approved as a front-line treatment for those with metastatic EGFR+ NSCLC and as an additional treatment for those who have tumor removal surgery for metastatic EGFR+ NSCLC.
Combination NSCLCtreatment of bemcentinib and pembrolizumab shows early promising results
Posted February 9, 2021
In an ongoing clinical trial, the combination treatment of bemcentinib (BGB324) and pembrolizumab (Keytruda®) in patients with checkpoint inhibitor (CPI)–naïve and CPI-refractory composite AXL-positive non–small cell lung cancer showed significant results. This is an important accomplishment since AXL receptors have been resistant to immunotherapy in other treatment types. The clinical trial is ongoing and seems promising in extending the efficacy of immunotherapy treatment.
Watch an explanation by Jonathan Thompson, MD, MS, Medical College of Wisconsin.
Addition of immunotherapies as a treatment for SCLC significantly improved patients’ overall survival
Posted February 8, 2021
Research presented at the International Association for the Study of Lung Cancer (IASLC) 2020 World Conference on Lung Cancer indicated an increase of overall survival rates in patients with small cell lung cancer (SCLC). This advantage is due to the increase of immunotherapy treatments for SCLC. Compared to historical standards of care, immunotherapy treatment has been extremely impactful in extending the life of those with SCLC.
LCRF Scientific Advisory Board member and former grantee Dr. Matthew Meyerson and colleagues recently published an article on the possible link between Latin American genetic ancestry and EGFR, KRAS lung cancer mutations.
Dr. Meyerson is Professor of Pathology at Dana-Farber Cancer Institute and Harvard Medical School; Director of the Center for Cancer Genome Discovery at DFCI; and Senior Associate Member of the Broad Institute. Download the paper here.
Team makes case for ICIs in early stage lung cancer
Posted October 26, 2020
Dr. Mark Kris
In a recent interview, Mark G. Kris, MD, of Memorial Sloan Kettering Cancer Center explained why he and his colleagues are discussing immune checkpoint inhibitors (ICIs) for early state lung cancers. “To cure more, we need better systemic therapies – adding ICIs to multimodal regimens can fill that need.”
Dr. Kris, a member of LCRF’s Scientific Advisory Board, spoke with MedPage Today for the ASCO Reading Room. Read the full interview here.
EGFR treatment continues to make strides
Posted September 25, 2020
Tagrisso® (osimertinib) remains one of the recurring highlights in the treatment of early-stage EFGR mutated non-small cell lung cancer. AstraZeneca presented new exploratory data at ESMO20 this week from the investigational Phase III ADAURA trial, showing, among other things, that 89% of patients who participated in the trial who were treated with Tagrisso remained alive and disease-free, compared to just 53% who received the placebo.
Dr. Roy Herbst
Roy S. Herbst, MD, Ph.D., chief of Medical Oncology at Yale Cancer Center and Smilow Cancer Hospital, New Haven, CT is principal investigator in the Phase III ADAURA trial and a member of the Lung Cancer Research Foundation Scientific Advisory Board.
AstraZeneca also shared new data at ESMO20 from its Phase III PACIFIC trial and Phase III CASPIAN trial. Read the full details: Biospace | Astrazeneca (Tagrisso®) | Astrazeneca (Imfinzi®)
Wildfires pose special risk for those with lung cancer
Dr. Karen Reckamp
Posted September 22, 2020
How worried should patients with lung cancer be about the air quality in areas of the country affected by wildfires? SurvivorNet asked LCRF Scientific Advisory Board member Dr. Karen Reckamp for her thoughts. Dr. Reckamp is Medical Oncology Director at Cedars Sinai.
“I think the air quality is a concern for anyone, [especially those] with any underlying lung disorders. There’s a huge concern for patients,” said Dr. Reckamp.
She recommended measures those in the Western US can take to protect themselves and their lungs. “The best thing that lung cancer patients can do is minimize their time spent outside. And if you have to be outside for some reason, things like [wearing] N95 masks can be helpful.”
Decrease in lung cancer cases not always positive, Dr. Stiles explains
Posted September 1, 2020
The National Cancer Institute is reporting a decrease in the number of lung cancer cases, but that’s not necessarily a good thing. Dr. Brendon Stiles, LCRF Board Chair, spoke with AM Buffalo about how we need to take COVID-19 into account when looking at current statistics. Current circumstances mean that more people are living with undiagnosed lung cancer and facing significant delays in treatment. Dr. Stiles went on to review common symptoms and underlined the importance of staying in touch with your primary care doctor. Watch the video below.
When clinical cancer trials fail to enroll a racially and ethnically diverse patient population, they run the risk of leaving critical gaps in understanding regarding the effectiveness of new approaches. That’s the conclusion of several reports on disparities in cancer mortality and access to clinical trials.
Dr. Narjust Duma, assistant professor of medicine and a thoracic oncologist at the University of Wisconsin Carbone Cancer Center, spoke with OncLive about this issue and the strategies healthcare organizations are using to enhance community relations and enroll a more racially diverse patient population in their clinical trials.
In an interview with OncLive, LCRF SAB member Dr. Mark G. Kris discussed how the treatment of patients with metastatic lung cancer today bears scant resemblance to what it was when he entered the field 4 decades ago.
Now, because of COVID-19, the lung cancer landscape is changing again. Dr. Kris, who is the William and Joy Ruane Chair in Thoracic Oncology at Memorial Sloan Kettering Cancer Center in New York, NY, learned on the fly how to continue treating patients when the region became an early epicenter of the pandemic.
“I think the message is, you can’t stop the delivery of care for people with lung cancers,” Dr. Kris said. “So, our challenge is, how do we continue to provide the same level of care and the right decision-making when there is this unbelievable force pervading everything?”
LCRF SAB member Dr. Karen Reckamp, director of the Division of Medical Oncology at Cedars-Sinai, spoke with Survivornet recently about COVID-19 risk in lung cancer patients. She pointed out that while lung cancer doesn’t make people more susceptible to coronovirus, compromised lung function means they could have a more severe reaction if they do contract the virus.
LCRF grantee Dr. Lecia V. Sequist from Massachusetts General Hospital was a panelist in a recent podcast on the results of the ADAURA trial, addressing the potential clinical and financial concerns of using osimertinib in the adjuvant setting in patients with EGFR-mutant NSCLC.
An international research effort is underway to assess the effects of lung cancer treatment on women’s sexual health. The Sexual Health Assessment in Women with Lung Cancer (SHAWL) will provide data to serve as the foundation for guidelines that can benefit patients worldwide.
Dr. Narjust Duma
“Sexual health correlates directly with quality of life. Studies in other cancers showed patients with sexual dysfunction have worse pain and worse symptom burden, and it also increases stress in their relationships,” said principal investigator Dr. Narjust Duma, assistant professor at the University of Wisconsin School of Medicine and Public Health and member of the medical oncology and lung cancer clinics at UW Carbone Cancer Center.
The effective design of so-called “umbrella” or “basket” clinical trials is increasingly important in the era of genome-driven cancer treatment. Drs. Alexander Drilon and Matthew Hellmann provide their perspectives on the largest such trial conducted in non-small cell lung cancer and recently reported in Nature. Dr. Drilon is a Lung Cancer Research Foundation grantee and has appeared on a recent #TogetherSeparately discussion of his work and FDA approvals.
The phase 3 ADAURA trial was big news at the virtual ASCO Annual Meeting held May 29-31. Physician Weekly interviewed the study’s principal investigator and presenter at ASCO, Dr. Roy Herbst, about the study and what’s next. Dr. Herbst serves on LCRF’s Scientific Advisory Board and is Ensign Professor of Medicine, Chief of Medical Oncology and Associate Director for Translational Research for Yale Comprehensive Cancer Center.
LCRF SAB member Dr. Mark Kris commented on recent practice-changing abstracts in lung cancer that were presented at the recent virtual 2020 ASCO meeting.
Phase 3 of the ADAURA trial concluded that 3 years of osimertinib following complete surgical resection and guideline-recommended adjuvant chemotherapy improves disease-free survival. “It shows important improvements in disease-free survival and does represent a new standard of care,” Dr. Kris said.
Dr. Jorge Gomez, medical director of the Thoracic Oncology Program and the World Trade Center oncology clinic at Mount Sinai Hospital, spoke with CURE® recently on why the Tecentriq approval is different and the importance of its expansion into patients with a high PD-L1 expression. Read more here.
Bruce Dunbar, a member of LCRF’s Board of Directors, was profiled on the Congressionally Directed Medical Research Programs (CDMRP) website in August 2021. Bruce was diagnosed with Stage IV ALK+ non-small cell lung cancer in 2017.
“My story is not that different from many others with NSCLC.” he recounted. “I was in the prime of my life, successful at work, loving every minute of raising my three then-teenaged daughters and, by all accounts, a picture of health. I was even training for the longest swim race of my life, a 7-mile event across Long Island Sound near my home just outside New York City. First, I thought it was just turning 50 and a few extra pounds that was slowing me down—then maybe asthma or an allergy. Treatment for that did not work, nor did it for pneumonia. More tests followed, along with more worry, more interruption, and, finally a diagnosis.”
Bruce serves as a Consumer Reviewer with the CDMRP’s Lung Cancer Research Program (LCRP). Read his story here.
Lung cancer is the leading cause of cancer death in women in the US, but a study in Chest (Pasquinelli et al.) suggests the 2021 United States Preventive Services Task Force (USPSTF) lung cancer screening guidelines, released in March, result in more women being ineligible for lung cancer screening than men.
Study researchers found that adding a specific risk prediction model criteria to the USPSTF guidelines may reduce this gender disparity in lung cancer screening. This risk prediction model does not feature an age-pack-years-quit-years restriction, but instead includes a total of 11 risk predictors.
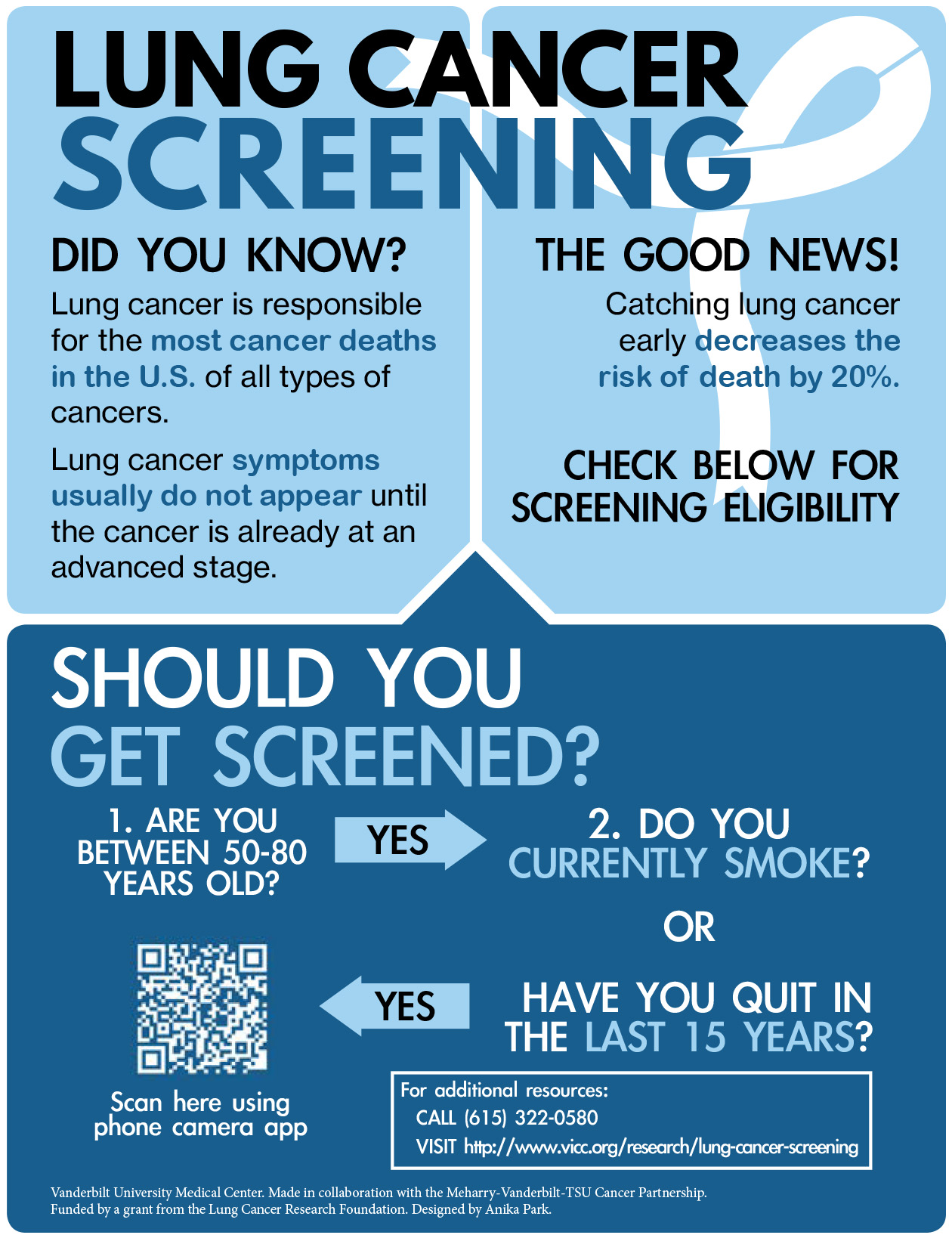
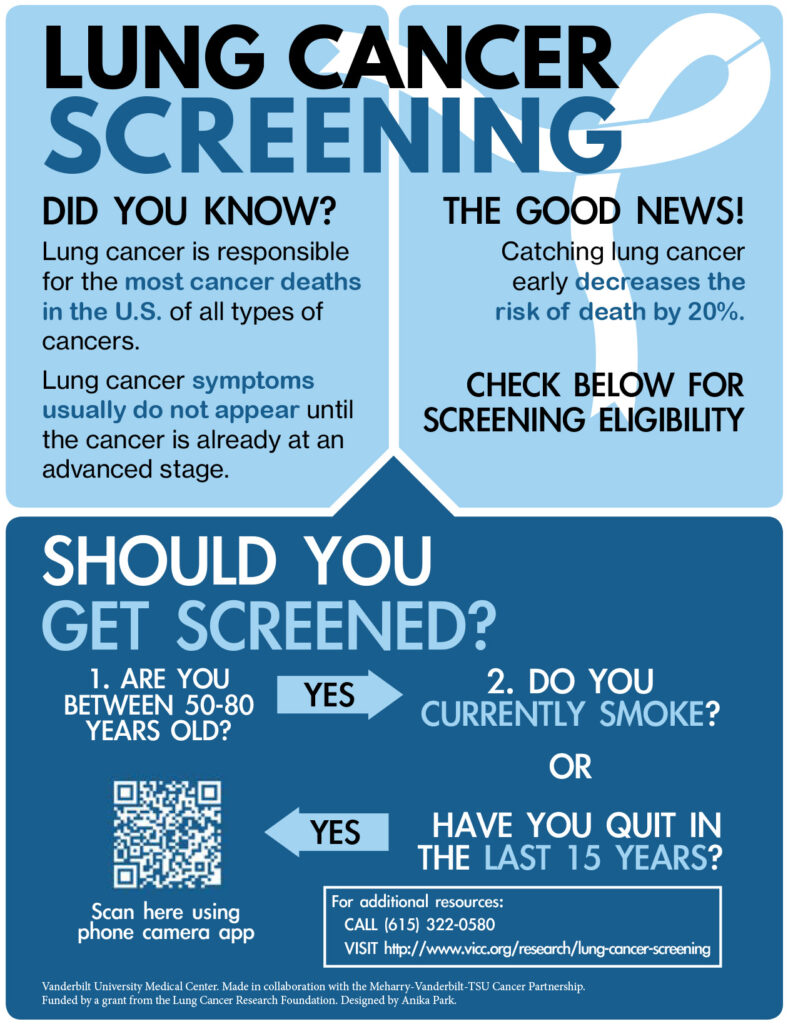
LCRF grantee Dr. Melinda Aldrich has developed a tool to communicate the importance of early detection of lung cancer. Dr. Aldrich, Associate Professor at Vanderbilt University Medical Center (VUMC) was awarded a 2019 LCRF Disparities Grant, and her research focuses on understanding differences in lung cancer risk and survival among different racial/ethnic populations. Her work also entails looking at genetic and non-genetic risk factors, the genetics of immunotherapy, and population genetics of African American and other admixed populations.
One of Dr. Aldrich’s grant objectives was to implement a community-engaged distribution strategy to build awareness around the importance of early detection of lung cancer. Collaborating with community partners across middle Tennessee and including input from Black and Latinx cancer survivors, she has developed an infographic. This infographic emphasizes the importance of lung cancer screening, describes eligibility criteria, and provides links to related resources.
My journey with Stage IV lung cancer started in early June when I started to feel dizzy and eventually developed double vision. I didn’t think it was out of the ordinary because I thought it was vertigo. Shortly after I started noticing that I would lose my balance, and began having issues swallowing. At this point I sought out medical attention at an urgent care and was told it was vertigo. I was sent home with some pills and told to come back in a week if there was no improvement.
The pills worked for a short amount of time but did not get rid of symptoms so I went back to urgent care for a second time. This time I was given steroids. A few days later I started noticing I was staggering to both sides when I was walking. At this point, I knew that an ER visit was warranted. Upon a multitude of tests and scans, there was a mass discovered in my lung. The neurologist admitted me to the hospital to complete an MRI scan – this scan revealed an additional mass in my brain stem. With this knowledge, I knew I needed to seek out the best possible care available and very quickly found my way to Penn Medicine, where I met with a doctor two days later.
The doctor at Penn Medicine confirmed that my diagnosis was Stage IV lung cancer. I was immediately admitted for further testing, scans, MRI, blood work, and a biopsy of the lung. The biopsy revealed that it was not small cell lung cancer. Upon waiting for the results of the biopsy, it was decided that the symptoms from the brain stem mass needed to be addressed immediately. The doctors put together a plan to do an outpatient procedure with gamma knife radiation.
While waiting for that procedure, the results of the blood test revealed that I had a marker for a genetic mutation called EGFR which had a targeted therapy available. The plan moving forward was to proceed with the gamma knife first and begin the targeted therapy the next day.
I am now in the recovery stages from my treatments and will be taking the targeted therapy once a day the rest of my life and continue with scans every three months in the near future. Through the donations of others to clinical research for targeted therapies, my journey has been made manageable and allowed for myself and millions of others’ lives to be saved.